Welcome to the tenth edition of FOI Clinical. Each week, we'll send you a briefing on outbreak news. When something urgent breaks, you'll get an alert the same day.
In this edition
Measles - Mumps - Vector-borne disease season: Chikungunya and West Nile virus - Plague update – Trichophyton mentagrophytes genotype VII update - H9N2 - Mpox
National interest
As of April 9, 2026, there have been 1,714 confirmed cases of measles this year, up 43 from last week's 1,671, the smallest weekly increase of 2026. Thirty-three states have reported cases.
The deceleration should not be mistaken for the end of the resurgence. South Carolina's outbreak is effectively over with no new cases, and Florida has slowed. But Utah continues to accelerate, and Oregon is seeing a new cluster of locally acquired cases with no clear epidemiologic links, suggesting undetected community spread.
- South Carolina: No new cases since the week of March 8. If this holds, the outbreak will be approximately one week from being declared over.
- Utah: 405 cases this year (602 for the outbreak). Case counts doubled week-over-week in late March, with exposure locations including Walmart stores, University of Utah buildings, clinics, and hospitals.
- Texas: 176 cases. 136 total cases in Hudspeth county, at least some of which are detention-associated).
- Florida: 144 cases as of April 4. The vast majority (106) in Collier County, most or all of which are presumably associated with the Ave Maria University outbreak.
- Arizona: 79 cases for 2026 (299 for the outbreak), with 14 new cases in March.
- North Dakota: 32 cases and 5 hospitalizations. After a lull, 6 new cases were reported in Ransom County.
- Oregon: 14 cases this year, 7 since the start of March.
Mumps
Maryland continues to drive national mumps numbers: 42 cases year-to-date according to NNDSS, representing 55% of the 76 cases reported nationally. Most Maryland cases are in adults in the Baltimore metropolitan area, according to a state communication from February For context, Maryland reported just 9 mumps cases to NNDSS in 2025.
Overall, mumps is tracking similarly to last year: 76 cases YTD compared to around 80 at the same point in 2025. A typical year sees 350–450 cases nationally.
Two doses of MMR vaccine are approximately 86% (range: 32% to 95%) effective against mumps, but protection wanes over time. Outbreaks among vaccinated young adults are well documented (e.g., Lewnard et al). CDC recommends a third dose of MMR for persons previously vaccinated with two doses who are at increased risk during an outbreak. Clinicians should consider mumps in adults presenting with parotitis or unexplained salivary gland swelling, even if fully vaccinated.
Vector-borne disease season
As spring temperatures arrive across much of the United States, so does the annual vector-borne disease (VBD) season. Mosquito- and tick-borne activity is lowest in winter, ramps up in late spring, and peaks from June through September in most of the country. Southern states, particularly along the Gulf Coast, see earlier onset and longer transmission windows.
The most commonly reported mosquito-borne diseases in the United States are dengue, West Nile virus (the leading cause of domestically acquired arboviral disease), and malaria.
Tick-borne diseases, especially Lyme disease, anaplasmosis, and babesiosis, are driven by a separate seasonal pattern tied to Ixodes tick activity, with nymphal ticks peaking in May–July across the Eastern seaboard and into the Midwest.
Prevention is centered on reducing exposure to vectors during peak transmission months. For mosquitoes, this includes the use of EPA-registered repellents, protective clothing, and limiting outdoor exposure during peak biting periods, alongside elimination of standing water around the home. For ticks, risk reduction relies on avoidance of high-risk habitats, use of permethrin-treated clothing or repellents, and prompt post-exposure tick checks and removal.
Two signals this early in the season are worth tracking:
Chikungunya
Chikungunya cases are running well above baseline. Through the week of April 4, there have been 137 cases reported nationally, compared to just 25 at the same point in 2025.
According to CDC, chikungunya is an acute viral illness marked by the abrupt onset of high fever and severe, often symmetric joint pain, typically 3–7 days after a mosquito bite. The joint pain, most commonly affecting the hands, wrists, ankles, and feet, can be debilitating.
Other symptoms include headache, myalgia, fatigue, and a maculopapular rash that usually appears a few days after fever onset. While illness is generally self-limited, some patients experience prolonged joint symptoms lasting weeks to months, occasionally progressing to a chronic inflammatory arthritis.
Severe disease is uncommon but can occur, particularly among older adults, neonates, and individuals with underlying medical conditions. Reported complications include neurologic involvement (e.g., encephalitis), myocarditis, hepatitis, and, rarely, multi-organ failure. Mortality is low but has been documented in large outbreaks.
While there is no specific antiviral treatment, a vaccine (Ixchiq) was approved by the FDA in November 2023 for adults 18+ at increased risk of exposure. Its use was paused in individuals ages 60+ in May 2025 so that a safety signal could be investigated. The pause was lifted in August.
West Nile virus
The Shelby County Health Department (Tennessee) confirmed one human case of West Nile virus (WNV) so far this year. This is early. WNV season in Tennessee typically peaks in August and September, with cases rarely reported before May.
Nationally, just 4 WNV cases have been reported through the week of April 4, which is within the normal range for this time of year (7 at the same point in 2025). West Nile caused 2,076 cases and 1,434 neuroinvasive cases in 2025.
Clinicians in the Mid-South should consider WNV in the differential for patients presenting with acute febrile illness, especially with neurologic symptoms (meningitis, encephalitis, acute flaccid paralysis). There is no vaccine or specific treatment for WNV.
Regional interest
Plague update
Apache County, Arizona confirmed a case of bubonic plague on April 7, the county's first human case since 2015. The patient was treated with antibiotics and has fully recovered. This follows the dog plague case in Santa Fe we covered in Issue 9.
Trichophyton mentagrophytes genotype VII update
Trichophyton mentagrophytes genotype VII (TMVII) is an emerging strain of dermatophyte fungus that causes tinea (ringworm). Unlike typical ringworm infections, which are commonly spread through casual skin-to-skin contact, contaminated surfaces, or animal exposure, TMVII appears to be transmitted primarily through sexual contact, with cases reported predominantly among men who have sex with men (MSM).
Clinically, TMVII infection presents as inflamed, painful, itchy, and often persistent skin lesions. The most commonly affected sites include the genitals, groin, buttocks, and perianal region, though facial involvement can also occur. Lesions are frequently atypical in appearance and may closely resemble other dermatologic conditions such as eczema, psoriasis, or secondary syphilis, which can lead to misdiagnosis and delays in appropriate treatment.
U.S. situation
The first U.S. case was identified in New York City in June 2024 in a man who reported multiple male sexual partners while traveling in Europe and California, followed by four additional cases in NYC through July 2024 (Zucker J et al., MMWR 2024). Since then, TMVII has been confirmed in a growing number of U.S. jurisdictions:
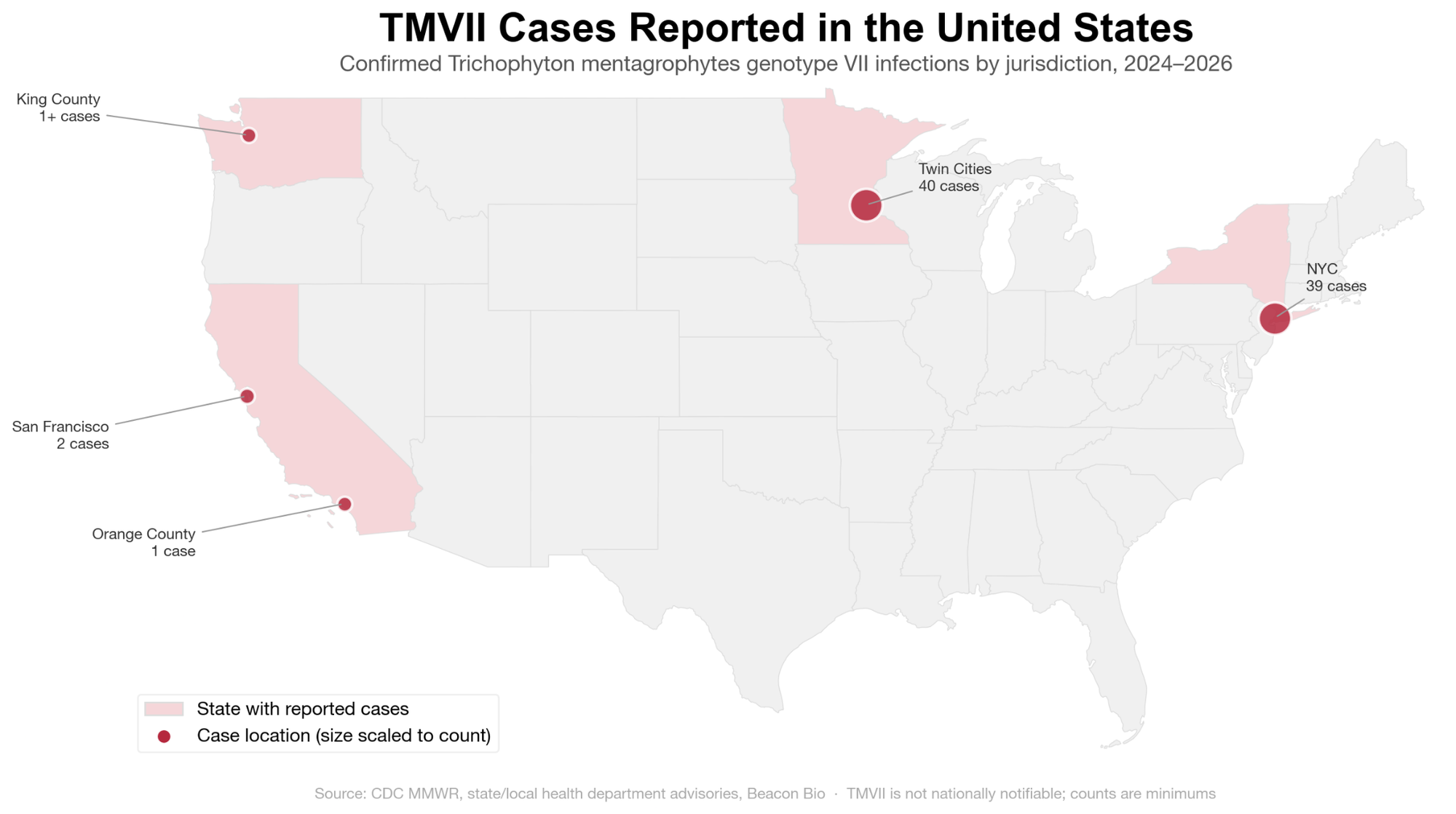
The Minnesota cluster is the largest documented U.S. outbreak, though this may reflect better surveillance rather than true case burden. Notably, neither San Francisco patient reported recent international travel, suggesting domestic transmission chains. The CDC notes that cases have been identified in "multiple U.S. cities" but the strain is "not yet widespread nationally." Because dermatophyte infections are not nationally notifiable, there is no comprehensive case count. The CDC maintains an Emerging Disease Registry for case reporting and offers clinical consultation ([email protected], 404-639-5168).
International interest
First H9N2 human case in Europe, additional cases in China
Italy's Ministry of Health confirmed the first human case of avian influenza A(H9N2) in the EU/EEA, reported by ECDC on March 25. The patient, in the Lombardy region, is a returning traveler from Senegal who was hospitalized. The patient has no known history of contact with poultry, according to WHO. Additional clinical details are limited.
In addition, two human cases were reported in China between March 27 and April 9, according to the World Health Organization. One case was in a child who became severely ill; the patient did not have a history of contact with poultry, but a family member did. The second case was in an older adult who recovered. A majority of human H9N2 cases have been reported in China.
Human-to-human transmission of H9N2 has never been definitively documented. ECDC assesses the risk to the general population as low.
Mpox update
Last week, we reported on the 39-case cluster of clade Ib mpox in Berlin, the largest cluster of locally acquired clade I cases outside Africa. Recently, CDC paused testing for more than two dozen pathogens, including mpox and rabies, removing assays from its public test directory on March 30. According to reporting from CIDRAP, state and commercial laboratories are absorbing the capacity; the Association of Public Health Laboratories estimates full restoration could take several months.