
This information is made available as a public service. To support our work and receive weekly updates on outbreak-prone disease activity, consider upgrading. We also have a general-reader publication, Force of Infection.
Tracking cyclosporiasis is more difficult than tracking some infectious diseases, because standard GI workups do not routinely include testing for cyclosporiasis. Typically, providers must suspect the diagnosis to order testing. This creates a detection bias that distorts surveillance, because it is sensitive to clinician awareness.
Michigan, for example, has a much higher number of cyclosporiasis cases at 2,640 than the second-most affected state, New York (470). This fivefold difference does not necessarily reflect a true difference in disease burden. A more likely explanation is that awareness of the outbreak is higher in Michigan which is driving a feedback loop. More awareness prompts more testing which leads to more detection and reporting.
When detection bias shapes surveillance data, our early impressions about outbreak timing and geography become unreliable. T0 get a clearer picture of the outbreak, I took a closer look at two independent data sources.
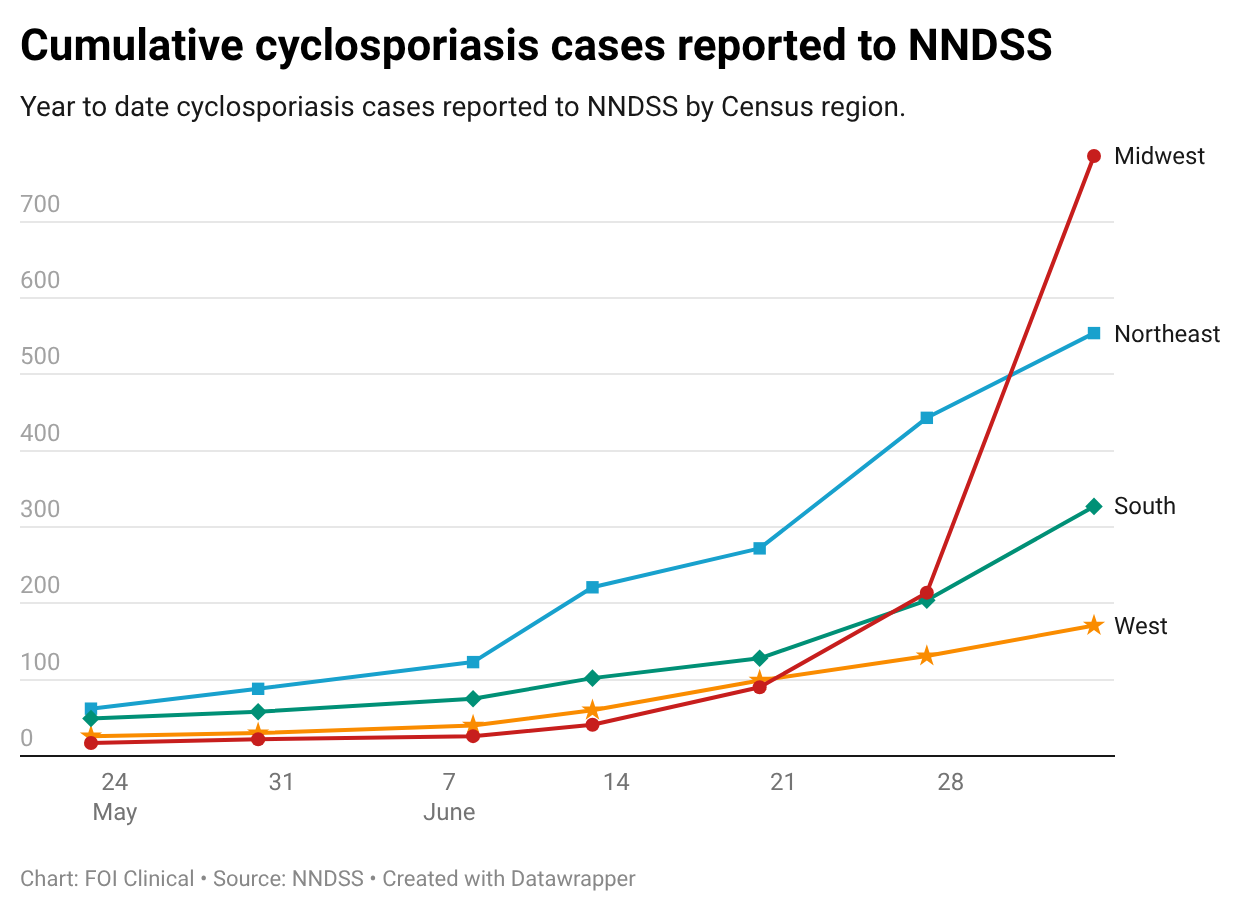
The National Notifiable Disease Surveillance System data tracks reportable diseases by state, on a weekly basis. Use of that data is how FOI Clinical was able to report on the outbreak beginning in our June 10 issue, much earlier than reported elsewhere. (Also our June 17, June 23, July 1 issues.) NNDSS data shows that cases began appearing in the Northeast in mid-May. The Midwest, by contrast, was the last region to report a notable increase during the week of June 6. This suggests that the outbreak has been underway longer than is widely understood, perhaps as long as two months.
A second line of evidence comes from data shared by BIOFIRE, which manufactures multiplex testing panels that screen for multiple GI pathogens simultaneously. The benefit of multiplex test data is it is not dependent on clinical suspicion. Test positivity for parasitic diseases began to rise sharply in mid-May, more than a month before the outbreak garnered widespread attention. This trend continues through today, confirming that the outbreak is still well underway.
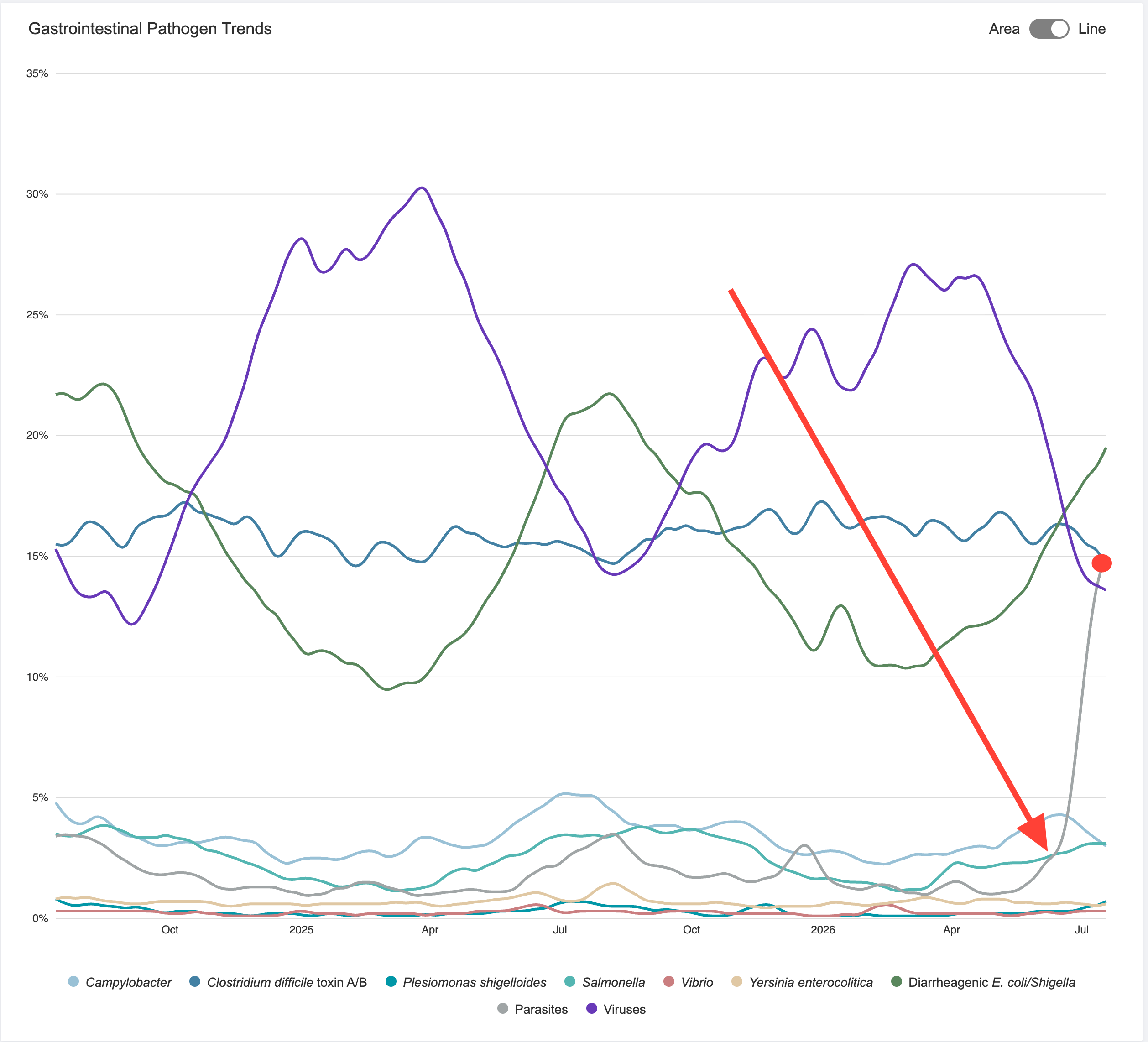
One important caveat: cyclosporiasis occurs annually in the United States during the May through August season. Some increase in cases and positive tests is expected this time of year. It is difficult to distinguish between a seasonal uptick in baseline transmission and a true outbreak. However, the magnitude of increase detected by BIOFIRE suggests something more than ordinary seasonal variation.
There are two conclusions.
First, reported cases are not a reliable map of outbreak burden. Geographic clustering reflects where providers are testing and reporting cyclosporiasis. It does not reliably indicate the true geographic distribution. An area with few or no reported cases might be affected, and an area with numerous reports may be reflecting greater awareness.
Second, the outbreak began earlier than has been widely recognized. Although media coverage has intensified only recently, both NNDSS and Biofire data support an onset date in May. The Northeast reported increased cases first, suggesting that geographic emphasis on the Midwest is a more recent development that may at least partly reflect detection bias.
Until the source is identified, clinical suspicion for cyclosporiasis should remain high across all regions, not just those with high case counts.
Related
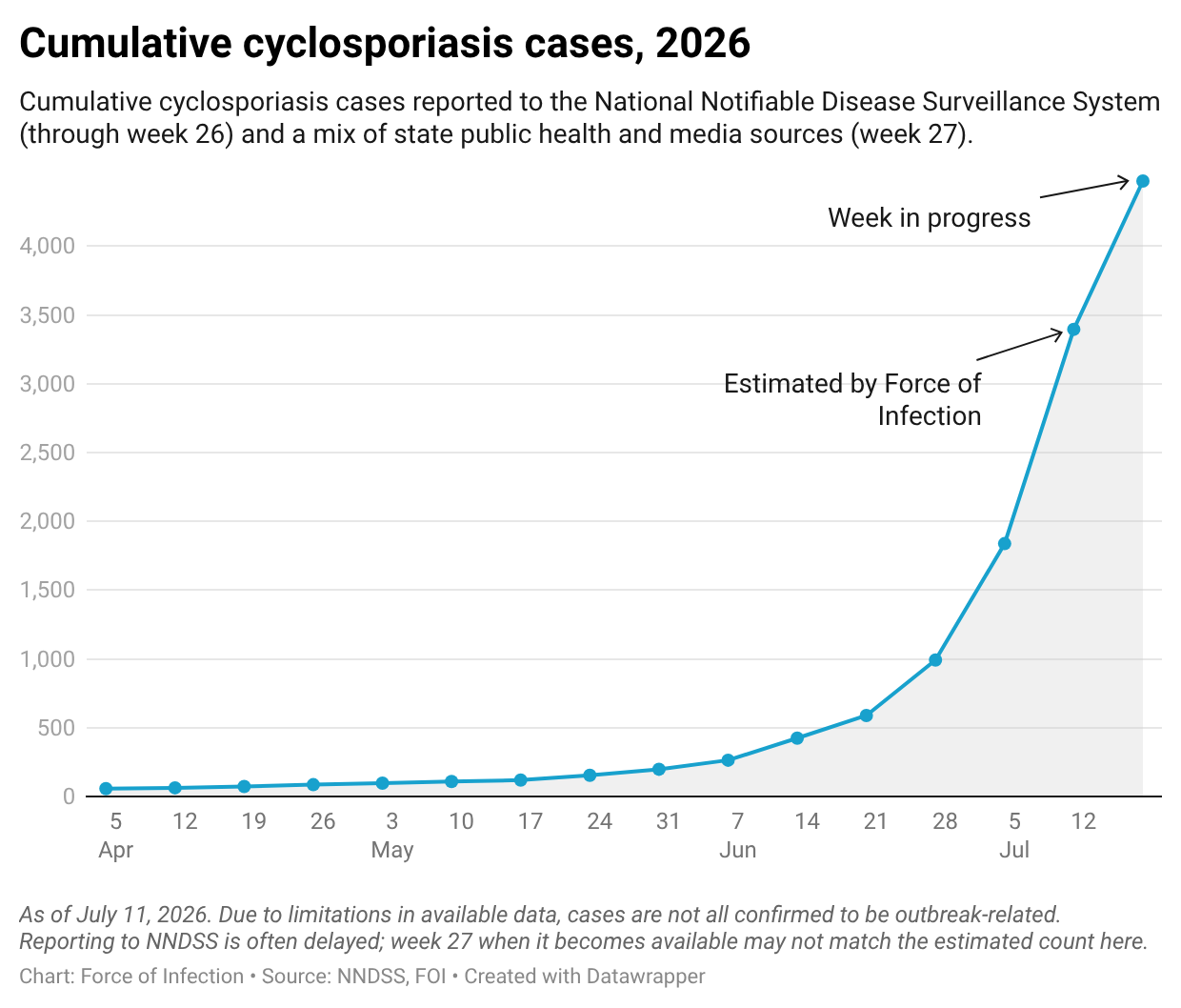
- Cyclosporiasis cases top 3,000. July 11 from FOI Clinical.
- Cyclospora cayetanensis: Multistate Outbreak with Midwest Epicenter. Comprehensive update on the outbreak, including diagnostic considerations and links to treatment recommendations. July 8 from FOI Clinical.
- A large cyclosporiasis outbreak is underway. An overview of the outbreak for a general audience. July 8 from Force of Infection.
- Clinical Guidance for Cyclosporiasis. CDC