
FOI Clinical issues two types of rapid communications: alerts for highest priority information, and advisories for emerging events clinicians should be aware of. This is an alert.
Situation Summary
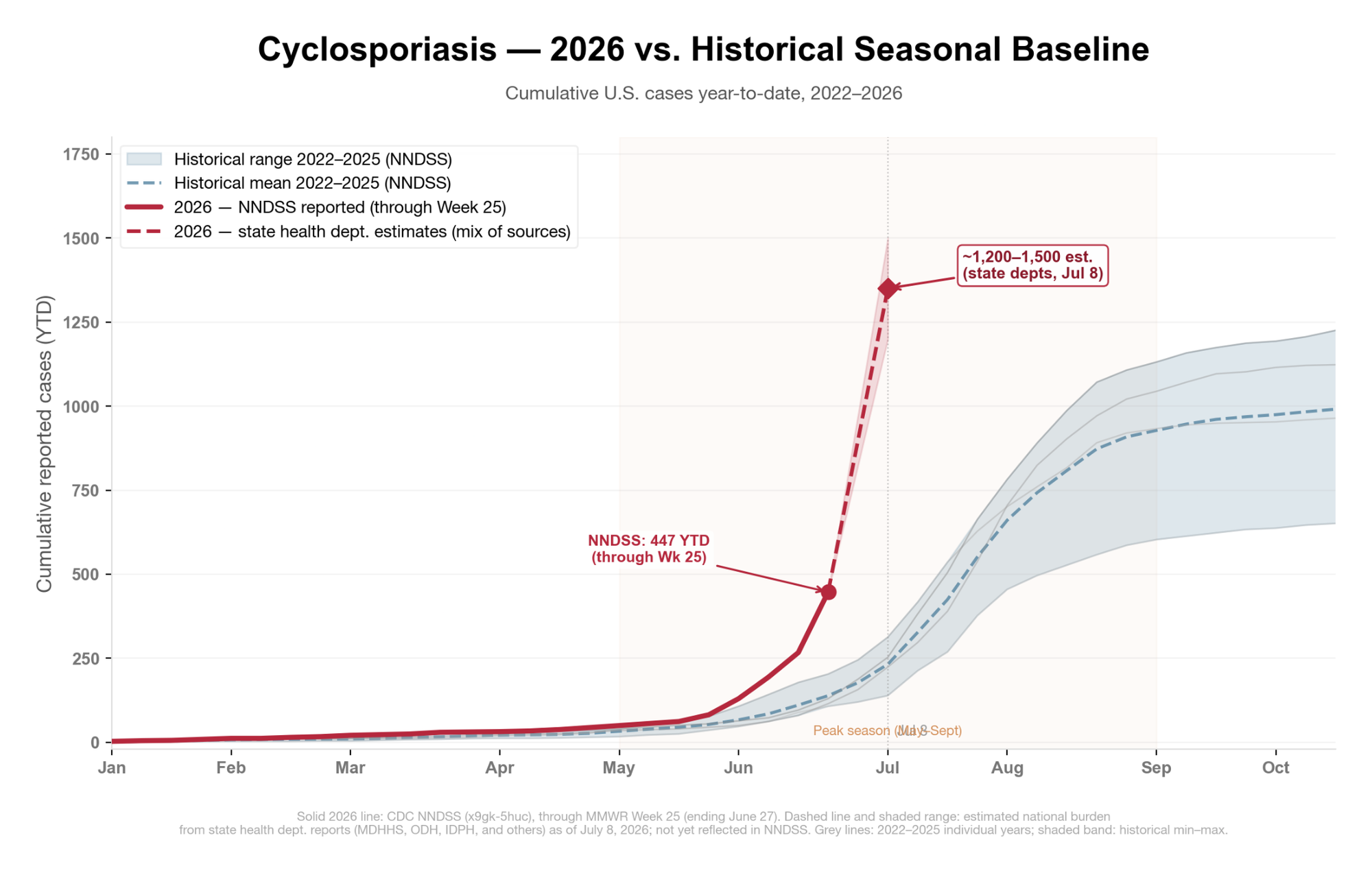
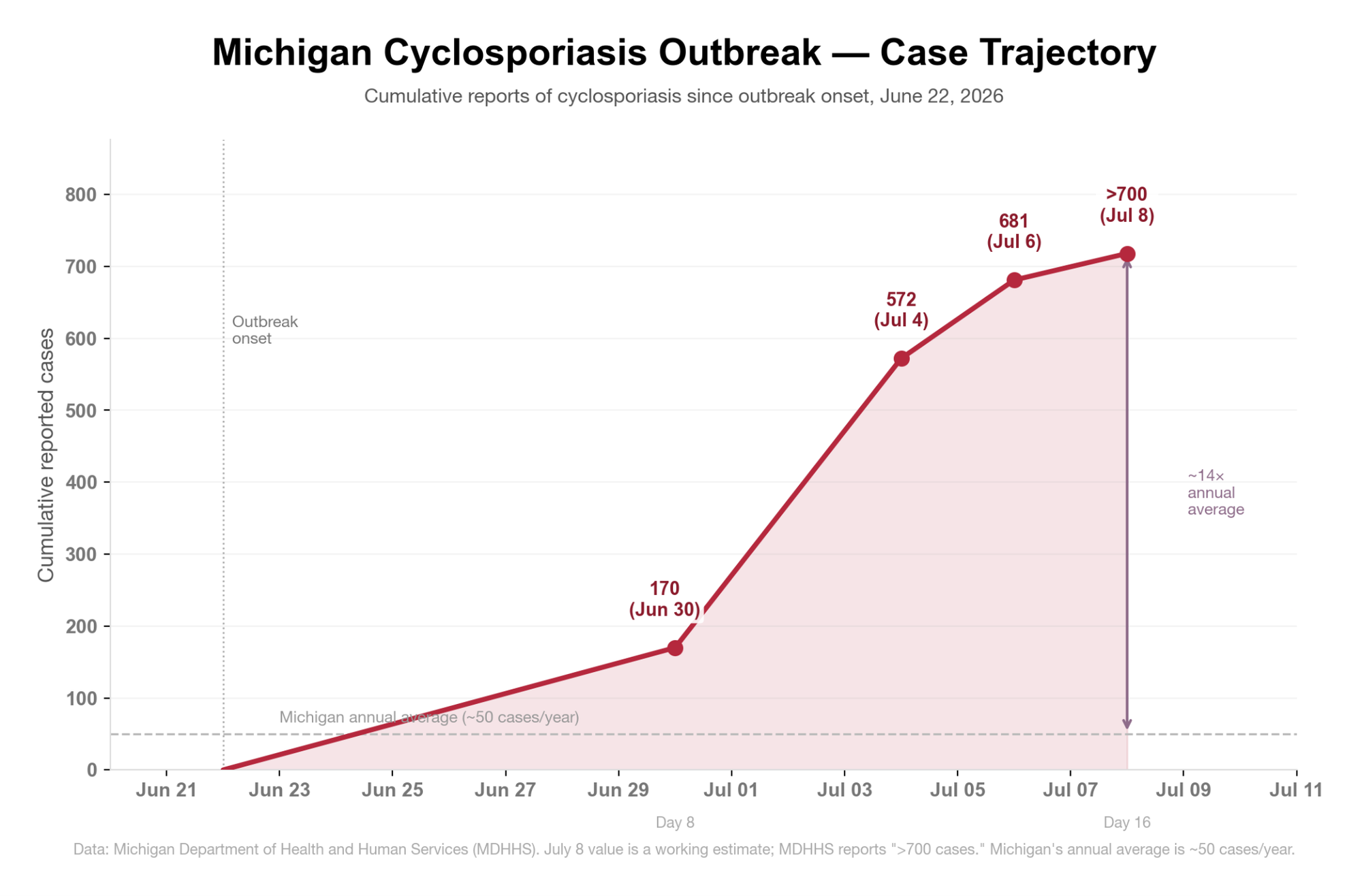
A rapidly expanding multistate Cyclospora cayetanensis outbreak has its epicenter in southeast Michigan and northwest Ohio, according to current reports. As of July 8, Michigan has received more than 700 reports of cyclosporiasis, including 38 hospitalizations since June 22. This is approximately 14 times the state's annual average. Ohio reports 177 cases across 43 counties (last updated July 7, per ODH spokesperson), with spread throughout central and northwest Ohio.
The effects extend beyond the Midwest. At least 18 states are affected nationally; aggregated state-level reporting suggests a true national burden well above 1,200 cases, far outstripping the CDC's most recent tally (145 cases as of June 16, now outdated).
No food source has been identified and no FDA recall has been issued. Traceback efforts to identify the source are underway.
Epidemiological Situation
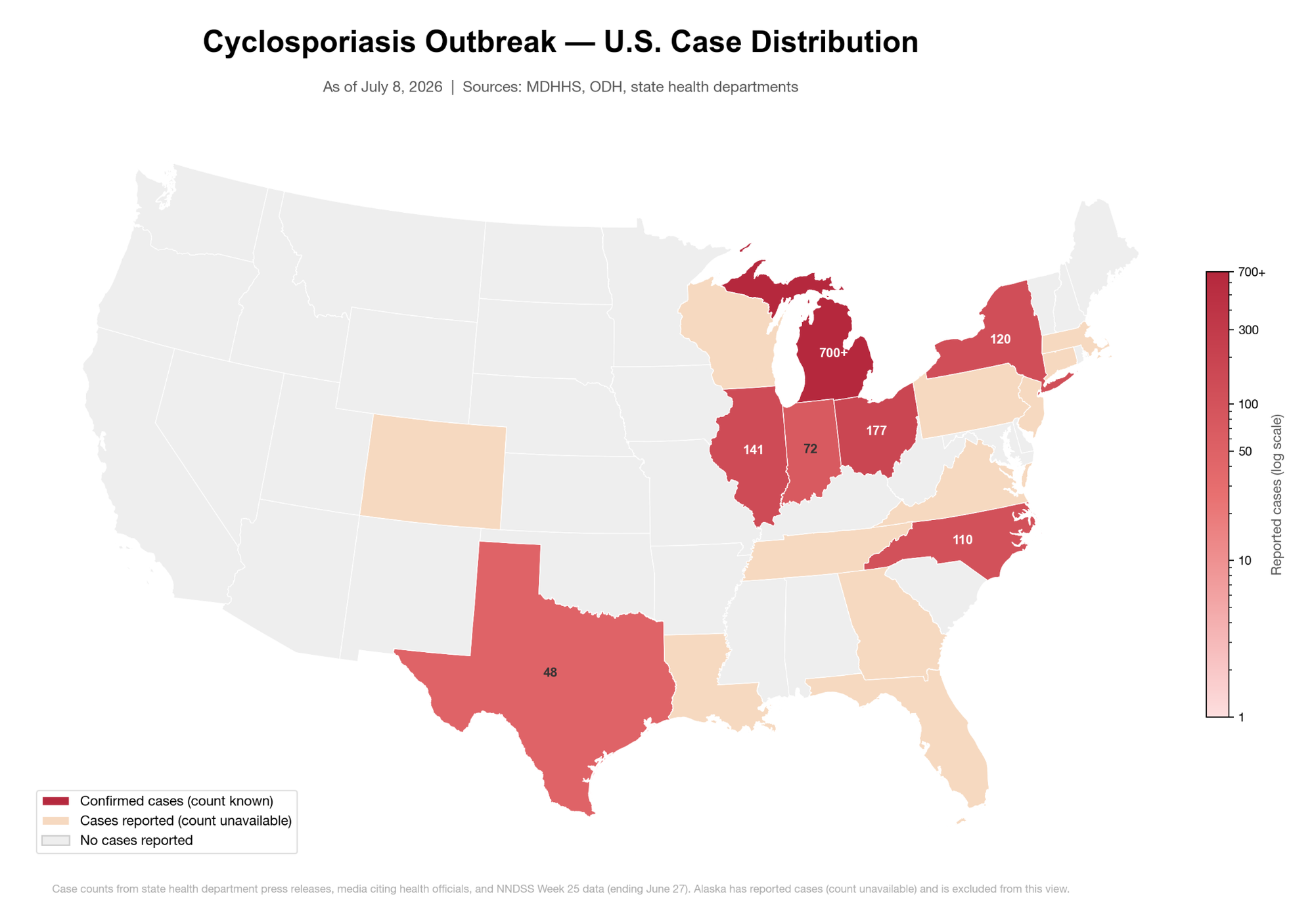
Case distribution (as of July 8, 2026)
Note on national totals: The CDC surveillance report (145 cases as of June 16) does not include more recent data. Michigan's >700 cases alone exceed the national CDC count by nearly 5-fold. Aggregated state health department data suggests a true national burden of at least 1,200 cases as of July 8.
| State | Cases | Hosp. | Last updated |
|---|---|---|---|
| Michigan | >700 | 38 | July 8 |
| Ohio | 177 | — | July 7 |
| Illinois | 141 | — | ~July 6 |
| New York | 120 | — | ~July 7 |
| North Carolina | 110+ | — | ~July 6 |
| Indiana | 72 | — | ~July 6 |
| Texas | 48 | 5 | ~July 6 |
| 11+ additional states | — | — | Various |
Michigan epicenter
Monroe County leads with 173 confirmed cases, followed by Washtenaw (95), Lenawee (86), and Wayne (58) counties. The ProMedica Health System, whose clinical footprint spans the Michigan-Ohio border, reports having treated 411+ confirmed Michigan cases. Illness onset has been concentrated since late June 2026.
Pathogen Background
Cyclospora cayetanensis is an intestinal coccidian protozoan parasite that infects the small intestinal epithelium, causing profuse watery diarrhea with a characteristic relapsing course. Transmission is exclusively fecal-oral via ingestion of food or water contaminated with sporulated oocysts. Person-to-person transmission does not occur. Cyclospora requires days to weeks of environmental sporulation before becoming infectious.
Previous U.S. outbreaks have been linked to fresh produce with complex supply chains, particularly:
- Bagged salad kits and mixed leafy greens
- Fresh basil and cilantro
- Raspberries
- Snow peas and scallions
Contamination typically occurs at the farm or irrigation level, making traceback investigations difficult. Cyclospora oocysts are resistant to standard chlorination and survive on produce that passes visual inspection.
Rinsing of produce is unlikely to be effective according to FDA, but is nonetheless recommended by CDC. A brief review of the literature by FOI Clinical found very little evidence. We conclude that washing may reduce but does not eliminate risk.
Clinical Guidance
Presentation
| Feature | Details |
|---|---|
| Incubation | 2–14+ days; average ~7 days |
| Cardinal symptom | Watery, often explosive diarrhea, frequent bowel movements, often debilitating at peak |
| Associated symptoms | Profound fatigue, anorexia, weight loss, low-grade fever, nausea, bloating, abdominal cramping |
| Course | Characteristically relapsing. Periods of relative improvement alternating with recurrence; may persist weeks to months untreated |
| Severity | Debilitating in immunocompetent hosts; substantially more severe in immunocompromised patients (HIV/AIDS with low CD4, organ transplant, active chemotherapy) |
The hallmark presentation is prolonged watery diarrhea with disproportionate fatigue and anorexia. Patients commonly present after weeks of symptoms, often having been told their workup was negative because standard stool panels do not test for Cyclospora (see Diagnosis below). Cyclosporiasis is commonly misdiagnosed as IBS, post-infectious IBS, or nonspecific colitis.
Diagnosis
The default panel for a standard stool workup at most U.S. institutions includes bacterial culture (Salmonella, Shigella, Campylobacter, E. coli), C. difficile testing, and an ova and parasite (O&P) examination. None of these reliably detect Cyclospora cayetanensis. Moreover:
- Routine stool wet preparation does not detect Cyclospora
- Standard O&P misses Cyclospora unless the lab specifically applies modified acid-fast staining or autofluorescence; most labs do not do this by default
- Bacterial stool culture does not detect Cyclospora
Thus, a negative standard stool workup does not exclude cyclosporiasis.
What to order
| Test | Notes |
|---|---|
| Modified acid-fast stain | Standard method; oocysts stain variably pink-to-red; must be explicitly requested |
| Cyclospora-specific PCR | Highly sensitive; must be explicitly ordered (not part of most routine panels) |
| BioFire FilmArray GI panel | Includes Cyclospora cayetanensis as a standard target (22-pathogen panel, FDA-cleared); reliable where available. Confirm with your lab whether it is in their panel configuration |
| UV fluorescence microscopy | Oocysts autofluoresce blue under 330–365 nm excitation, green under 450–490 nm; available at reference labs. Do not use iodine in wet-mount preparations as it impairs autofluorescence. |
Communicate directly with the laboratory. When ordering stool O&P, write e.g., "Evaluate for Cyclospora cayetanensis; please apply modified acid-fast staining." Oocysts may be shed intermittently; multiple specimens increase sensitivity.
Treatment
| Scenario | Regimen |
|---|---|
| Immunocompetent adults | TMP-SMX DS (160/800 mg) PO twice daily × 7–10 days Link to more info |
| Immunocompromised patients | Profoundly immunocompromised patients (AIDS, transplant recipients) may require a longer course and/or higher dose of TMP-SMX. Acute infection is usually followed by long-term suppressive therapy (TMP-SMX DS 3 times weekly) to prevent relapse. Infectious disease consultation recommended. Link to more info |
| Sulfa-allergic patients | Nitazoxanide or ciprofloxacin are recommended for patients unable to take TMP-SMX due to sulfa allergy, although treatment failure may occur. Nitazoxanide efficacy reported at 71–87%; ciprofloxacin is a suitable alternative but less effective than TMP-SMX. Infectious disease consultation recommended. Link to more info |
| Pediatric patients | Pediatric patients ≥2 months to 18 years: 8–10 mg/kg TMP and 40–50 mg/kg SMX per day, orally, in 2 divided doses for 7–10 days. Link to more info |
| Supportive care | Oral rehydration. |
Action Items for Clinicians
1. Order the appropriate test. For any patient with prolonged (>3–5 days) watery diarrhea, particularly with disproportionate fatigue, anorexia, or a relapsing course, order modified acid-fast staining or Cyclospora-specific PCR explicitly. Do not rely on a negative standard O&P.
2. Take a detailed dietary history. Until a source is identified, document consumption of fresh leafy greens, herbs (basil, cilantro), raspberries, snow peas, and scallions in the 1–14 days before symptom onset. Share findings with public health during case investigation.
3. Treat confirmed cases promptly. The absence of a recall does not lower the clinical probability of cyclosporiasis in patients with compatible presentations. Treat with TMP-SMX DS without waiting for an outbreak source to be named.
4. Report confirmed cases. Cyclosporiasis is nationally notifiable in 47 states, the District of Columbia, and New York City. Report to your state or local health department promptly and retain specimens for genotyping. Timely reporting is essential to the ongoing traceback investigation.
5. Counsel patients on produce handling. Until a specific source is identified, advise avoiding or cooking fresh produce, including herbs and leafy greens. Cooking destroys Cyclospora oocysts; it’s unclear whether rinsing is effective.